Low Back Pain
|
||||||


Introduction
Physical therapy in Western Springs for Lower Back
Welcome to Clarity Physical Therapy & Wellness Center's patient resource about low back pain.
Low back (lumbar) pain is one of the main reasons people visit their doctor. For adults over 40, it ranks third as a major issue—after heart disease and arthritis— that necessitates medical treatment.
Eighty percent of people will experience low back pain at some point in their lives. Furthermore, nearly each individual who suffers from this problem will endure recurring low back pain.
Very few people who feel pain in their low back have a serious medical problem! Ninety percent of people who experience low back pain typically report that their symptoms usually resolve in 2-6 weeks. In addition, experiencing a bout of back pain does not usually mean your condition will develop into a chronic back issue.
For moderate or severe pain that persists or becomes debilitating, the temporary use of pain relievers and physical therapy may help provide lasting relief.
This guide will help you understand:
- The anatomy of the spine and low back
- What causes low back pain
- What the most common symptoms are
- How health care professionals diagnose back pain
- how to manage your pain and prevent future problems
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Back Pain|limit:15|heading:Hear from some of our patients who we treated for *Back Pain*#
Anatomy
What Makes Up the Lumbar Spine?
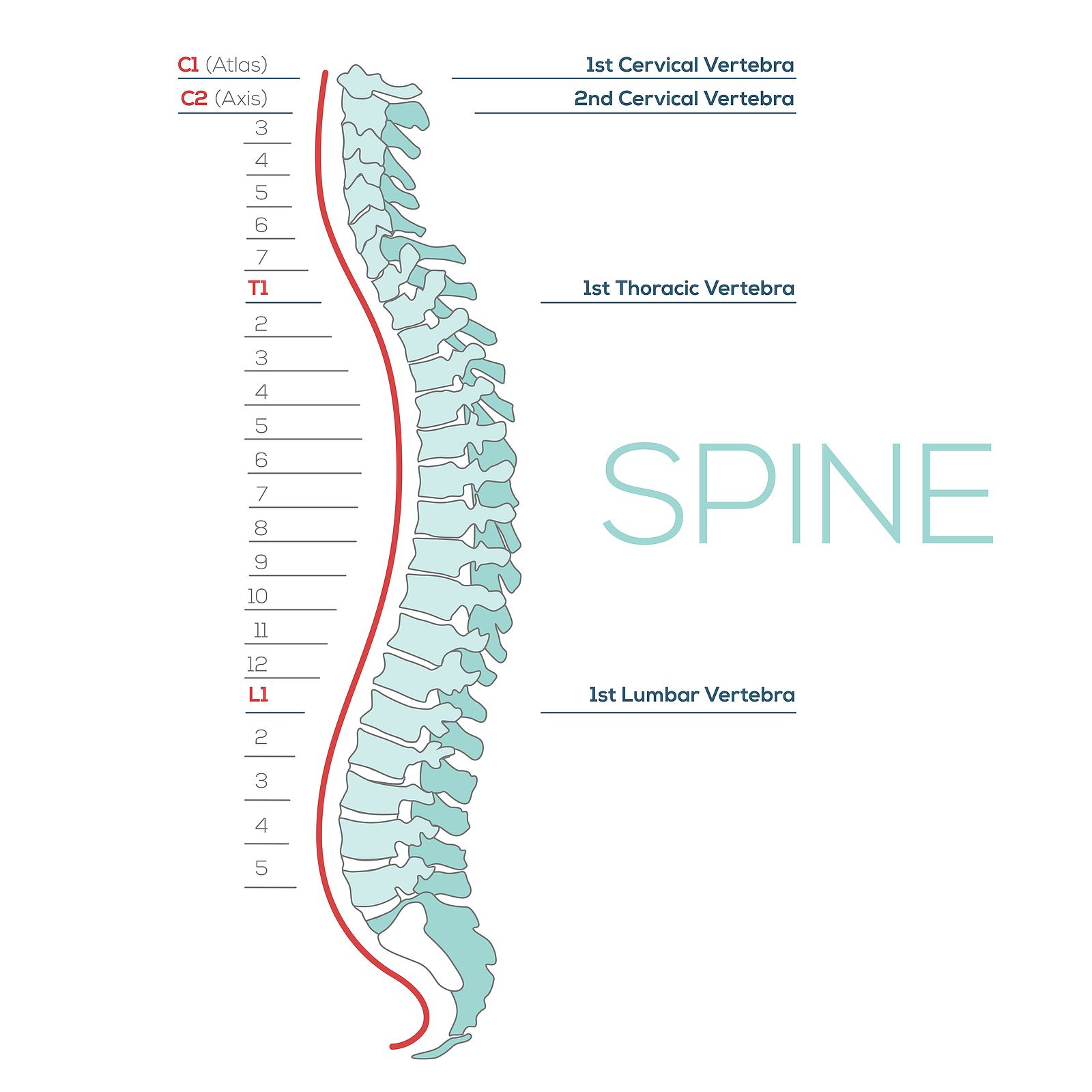
The human spine is made up of 24 spinal bones, called vertebrae, as well as the sacrum and the coccyx. The sacrum is a triangular bone near the bottom of the spine and the coccyx is more commonly known as the tailbone.
Vertebrae are stacked on top of one another to create the spinal column. The spinal column gives the body its form and helps sustain an upright position.
The lumbar spine—where pain is often experienced—is made up of five vertebrae positioned near the bottom of the spinal column. Doctors often refer to these vertebrae as levels L1, L2, L3, L4 and L5. The ‘L’ refers to ‘lumbar’. The lowest vertebra, L5, is connected to the top of the sacrum—a triangular bone at the base of the spine that is located between the two pelvic bones. Some people are born with an extra or sixth lumbar vertebra called L6. Having an extra vertebra doesn't usually cause physical problems.
The main portion of a vertebra is a circular segment of bone called a vertebral body. This structure supports about 80% of the body's weight load while an individual is standing. Vertebral bodies are also the point of contact or attachment for the spinal discs located between vertebrae. The lumbar vertebral bodies are taller and bulkier than the vertebrae in the cervical and thoracic regions because the lower back is designed to withstand more pressure and weight during daily activities such as lifting, carrying, and twisting. The bulkier vertebral bodies also provide support that allows the large, powerful muscles attached to or near the lumbar spine to work effectively.
The second portion of the vertebra is a body protrusion called the spinous process. This is that hard bony structure you feel when you run your fingers down the back of your spine. The vertebral body and the spinous process are joined together by vertebral arches. The arches form a ring that enclose the spinal cord and cerebrospinal fluid. Vertebrae are also connected by fibrous facet joints that are located on each side of the spine. The joints improve the stability and flexibility of the spine. The stacked formation of vertebrae along the spinal column forms a long, hollow tube that protects the spinal cord.
The spinal cord originates at the base of the brain and travels down the spine through the hollow tube formed by the vertebral arches into the L2 vertebra. Below this level is a bundle of nerves that further extend downward and travel to the pelvic organs and lower limbs. This bundle of nerves is called the cauda equina. In Latin, this term means ‘horse’s tail’ because it resembles the strands of a horse’s tail.

The spinal cord also consists of nerve roots that extend from the sides of vertebrae. Networks of nerve roots allow long nerve fibers to travel throughout the body and form the body’s electrical system. The nerve roots and fibers along the cervical spine extend to the neck, shoulders, arms, and hands. The nerves in the thoracic spine travel into the chest and abdomen. Nerve roots that originate in the lumbar spine consist of nerve fibers that travel to the lower regions of the body such as the pelvis, hips, thighs, legs, and feet.
How the Spine Works
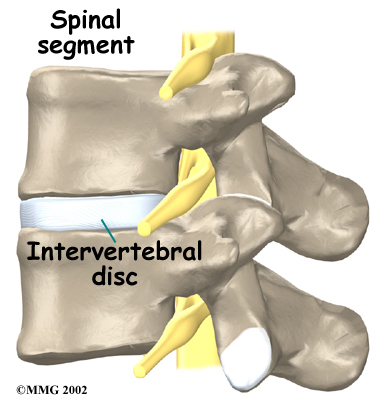
It is sometimes easier to understand how the spine works by looking at a spinal segment. A spinal segment consists of two vertebrae separated by an intervertebral disc, the nerves that leave the spinal cord at that level, and the small facet joints that link each level of the spinal column together.
The intervertebral discs normally work like shock absorbers. They protect the spine against the daily pull of gravity. They also cushion the spine during strenuous activities that put extensive pressure on the spine, such as jumping, running, and lifting.
An intervertebral disc is made up of two parts. The center, called the nucleus pulposus, is spongy and provides most of the disc's ability to absorb shock. The spongy center is also designed to transmit force and resist rotation. The nucleus pulposus is held in place by the annulus, which is found on the outside of the disc. The annulus is a series of strong ligamentous rings. Ligaments are strong connective tissues that attach bones to other bones. These ligaments form a criss-cross layer of protective tissue around the middle of the disc (the nucleus pulposus). The criss-cross formation is significant, as only half of the ligaments engage when the spine rotates to one side, while the ligaments on the opposite side remain stationary. The same activity occurs when the spine is rotated in a different direction. The criss-cross structure of the ligaments that make up the annulus provide maximum support, resistance, and flexibility of the spine.
There are also two facet joints—one on each side of the spine—that connect two stacked vertebrae in a spinal segment. Facet joints are located along the sides of the entire spine, from the neck down to the sacrum. The pattern and alignment of the facet joints in the lumbar region allow the spine to easily bend forward and backward. The anatomy of the lumbar spine also allows a certain degree of rotation, but not as much as the spinal segments in the cervical or thoracic spine. As the lumbar spine rotates, the facet joints squeeze together on one side and slightly expand on the other side to facilitate spinal movement.
The surfaces of the facet joints are covered by articular cartilage. Articular cartilage is smooth, rubbery tissue that covers the ends of most joints. It allows the ends of bones to move against each other smoothly without causing painful friction between bones that come in contact with one another.
In addition to facet joints on the sides of the spine, there are two spinal nerve roots that exit the sides of each spinal segment, one on the left and one on the right. As the nerve roots leave the spinal cord, they pass through a small bony tunnel on each side of the vertebra, called a neural foramen.
Spinal segments along the entire spine, including the lumbar spine, are heavily supported by ligaments and muscles that tremendously reinforce their strength capabilities. Ligaments—that enhance stability by attaching bones to bones—are arranged in various layers and run in multiple directions. Thick ligaments connect the bones of the lumbar spine to the pelvis and the sacrum (the bone below L5).
The muscles of the lower back are also arranged in layers. The deepest layer of muscles is located along the back surface of the vertebrae. These deep muscles coordinate their actions with the muscles in the abdomen (the core) to help hold the spine steady during activity.
A specific group of muscles called the erector spinae muscles also make up one layer of the lower back muscles. These long muscles run up and down the spine, from the chest and lower ribs down to the bottom of the back. You can easily feel your erector spinae muscles at the bottom of your back protrude outward slightly if you stand on one foot and then lift one leg backward. The long muscles twist together in the lumbar spine to form a thick, wide tendon sheath near the bottom of your back—called fascia—that connects the bones of the low back, pelvis, and sacrum. This fascia provides substantial support for the lumbar spine, especially when the spine bends forward.
Causes
Why do I have low back pain?
There are many causes of low back pain and health care professionals are not always able to pinpoint the exact source of each patient's pain. Although the exact cause of the pain may be hard to accurately identify, most back pain can be effectively treated based on symptoms and knowledge about how structures in the back and spine usually respond to certain activities.
Acute tissue damage, such as a torn muscle, an irritated disc, a pulled ligament, or a spinal fracture will cause acute (short-term) back pain. Most back pain of this nature usually heals within 6-12 weeks of the injury. For some individuals, the recovery period may be shorter than six weeks. Repetitive activities of daily living, when performed correctly, actually keep the spine strong! However, inactivity, prolonged sitting, or repetitive heavy loading with improper mechanics or poor efficiency can mean the lumbar spine is subjected to more load, rotation, or strain than it can normally withstand. This type of issue can lead to an acute injury, or more localized degeneration (wear and tear) than would typically occur with age. Gradual degeneration of back and spinal tissue does occur with age, but the aging process alone is not usually the direct cause of back pain. Persistent or chronic back pain may also be associated with other contributing factors such as systemic inflammation, stress, tension, or fatigue.
There is strong evidence that smoking cigarettes, for example, accelerates degeneration of the spine, specifically the flat part of the vertebrae called the vertebral endplate. This can cause a vacuum type of phenomenon in which the intervertebral disc begins to shrink or be pulled inward against a vertebra, causing decreased disc height between the vertebrae. Scientists have also observed hereditary links among family members, which shows that genetics plays a role in how fast degenerative changes in the spine may occur.
Degeneration
Under healthy conditions, the intervertebral disc adapts to different spinal movements. The disc is spongy and firm, and like most cartilage it actually gets stronger in response to increasing loads! Health care professionals used to believe that cartilage damage was caused by a “wear and tear” issue, but now understand that it is actually a “wear and repair” phenomenon where the body’s natural repair processes may weaken over time. This means you should not be afraid of increasing the load on your spine when proper mechanics are used. Furthermore, the nucleus in the center of the disc contains a great deal of water. This gives the disc its ability to absorb shock and help the spine withstand heavy and repeated forces.
Normal structural changes in the disc occur with age, but this does not typically lead to pain. However, the annulus that surrounds the nucleus of the disc weakens and begins to develop small cracks and tears over time. The disc also begins to lose some of its protective fluid, causing it to shrink in size and height. As the disc continues to degenerate, the space between the vertebrae decreases. This compresses the facet joints along the back of the spinal column. As these joints are forced together, extra pressure builds on the articular cartilage on the surface of the facet joints. In combination with local or systemic inflammation, this extra pressure can damage and sensitize the facet joints. If this issue progresses, arthritis may develop in the facet joints.
These degenerative changes in the discs, facet joints, and ligaments may cause the spinal segments to move more than they usually do, requiring the muscles to work harder to distribute force and keep the spinal column supple and strong. Extra movement is not always an issue, however—think of a gymnast’s or circus performer’s degree of spinal mobility! Nonetheless, extra movement within the bones and ligaments without strong, supple, conditioned muscles may lead to poor force distribution and frequent episodes of muscle, joint, or ligament sprain.
In some cases of degeneration, the nucleus of the disc may push through a torn annulus, toward or into the spinal canal, or into the space where the spinal nerves are located. This is called a herniated or ruptured disc. Sometimes patients refer to this as a slipped disc. The disc material that squeezes out may directly press against the spinal nerves. The disc tissue that pushes through also releases enzymes and chemicals that produce inflammation in the area. The inflammation caused by the chemicals released from the disc often, but not always, causes the transfer of pain signals to the brain. Pressure on the nerves may cause additional sensitization or breakdown of the protective sheath around the nerves.
As the degeneration continues, the body naturally tries to adjust to the disc damage as well as the extra motion the degeneration is causing. In response to the extra movement, the body may develop bony outgrowths around the edges of the disc and facet joints to try to redistribute the load and make the joint more stable. These bony outgrowths are called bone spurs, or on an x-ray report they may be referred to as osteophytes or facet hypertrophy. These bone spurs may not cause symptoms or they may create nerve sensitivity by pressing on the nerves and blood vessels in the spine as they pass through the opening in the vertebra (neural foramina). Bone spurs may also limit normal motion. In addition, the pressure around the nerves may cause pain, numbness, and weakness in the lower back, buttocks, lower limbs, and feet.
Over time, a spinal segment that has degenerated and become more mobile (as described above) eventually becomes stiffer and even less mobile. The ligaments thicken, facet joints enlarge, and disc tissue dehydrates in a continued attempt to adapt to the structural changes and maintain efficient force distribution. Typically, a stiff spinal segment doesn't cause as much pain as a segment that moves around too much. As a result, this stage of degeneration may actually lead to pain relief for some people.
Understanding Types of Pain
Pain research is ever-evolving. The most current guidelines divide pain into a few key categories. The key message is that although pain is a complex perception, all pain is real. It’s a form of signal output from the brain in response to messages from the body. The full definition states that pain is an unpleasant sensory and emotional experience associated with or resembling that associated with actual or potential tissue damage. Back pain commonly falls into all the categories below, which can help explain what may be causing low back pain,, why back pain is so intense at times, or why it lingers.
Nociceptive Pain
This is pain that is produced in proportion to the messages coming to the brain from the tissues that are irritated, damaged, inflamed, or are experiencing mechanical overload. For example, you would expect to feel immediate pain after dropping something heavy on your foot, but it should resolve in a reasonable amount of time if serious damage did not occur. This pain also generally follows a predictable pattern, such as the pain you feel after an acute back muscle spasm. Your back may feel fine while sitting down, but may begin to hurt when you transition to standing. The pain may be milder in the morning and predictably stronger in the evening or following certain activities. The key feature of this type of pain is that it doesn’t last beyond 12 weeks—even though that might not be what your experience feels like.
Neuropathic Pain
This type of pain arises from specific damage or the disruption of the somatosensory system, which is the network of nerves throughout the brain and body that allow you to sense touch, temperature, muscle stretching, and body position. This system is also responsible for taste, hearing, vision, and smell. When neuropathic pain develops, it may be a prolonged experience beyond 12 weeks, where signal transfer to and from the brain gets disrupted. Irritated nerves can also become so sensitive that they may stimulate pain signals in the absence of new tissue damage. Fears and emotions can also contribute to this type of pain, but that isn’t always the case. In cases of low back pain, neuropathic pain occurs when a nerve exiting the spinal column gets inflamed or damaged. Most of the time, the pain will travel down the legs along the path of the nerves involved.
Central Sensitivity or (Nociplastic Pain)
This type of pain arises from altered perception of the messages coming from the body, despite there being no clear evidence of actual or threatened tissue damage, or clear evidence of a disease or disruption of the body’s sensory system (the somatosensory system). This pain is very real, it’s just not necessarily coming from newly damaged tissue or an area that hasn’t healed properly. This type of pain often occurs in the back and usually lasts longer than 12-16 weeks. It is believed that messages from the body that normally wouldn’t create a pain response become amplified within the central nervous system (CNS). These types of pain signals are strongly influenced by thoughts, fears, perceptions, emotions, and environmental triggers. There is also strong evidence that individuals with neuropathic pain will have elements of central sensitization (nociplastic pain) as well.
Many patients with back pain may have a mix of two or more of the types above.
The good news is that all types of pain typically respond to treatment. A health care professional needs to recommend the appropriate form of treatment for the type of pain you are experiencing!
Spine Conditions
Common Spinal Conditions
Complications from back injuries or spinal degeneration can lead to specific spinal conditions. These include:
- Annular tears
- Internal disc disruption
- Herniated disc
- Facet joint arthritis
- Segmental instability
- Spinal stenosis
- Foraminal stenosis
Annular Tears
The structure of our intervertebral discs change with age, much like our hair turns gray. Perhaps the earliest stage of degeneration occurs due to tears that occur in the annulus. These tears can result from natural tissue changes over a period of time or they can be the result of a sudden injury to the disc due to an awkward twist or increased strain on the disc that leads to damage of the annulus. Annular tears may cause pain in the lower back until they heal and form scar tissue.
Internal Disc Disruption
Multiple annular tears can lead to a weakened disc. Furthermore, the disc that sits between two vertebrae naturally dehydrates and shrinks in size (height) over time. This process can accelerate due to a cumulative injury. A cumulative injury is a work-related injury that develops due to repetitive movements. The loss of disc height causes the vertebrae to compress closer to one another. The collapsing disc may be a source of pain because it has lost the ability to offer efficient shock absorption between the vertebrae—a condition known as internal disc disruption. This type of problem primarily causes mechanical back pain due to inflammation of the disc and surrounding structures. However, the disruption of the normal disc anatomy can also add pressure to the nerves in the area and may result in neuropathic pain. In many cases, the body reacts to a collapsed disc by growing small bony outgrowths (bone spurs) near the edge of the disc or the small joints nearby (facet joints) to contain the splaying of the disc. Bone spurs can cause pain by pressing on nearby nerves, blocking their passage, or squeezing nerve roots when an individual tries to move the back naturally.
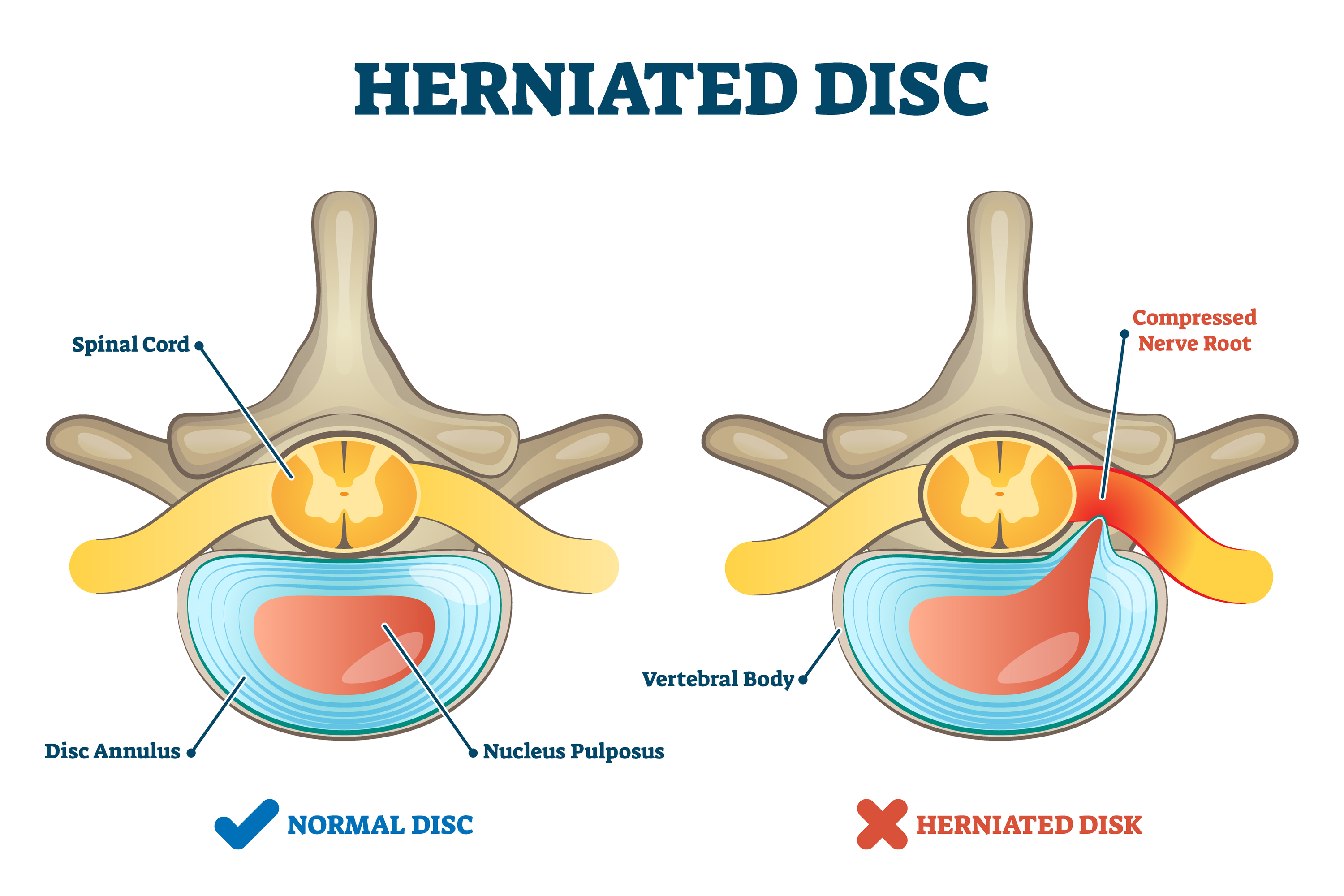
Herniated Disc
A weakened disc may herniate (shift out of place) or eventually rupture. If the annulus of the disc tears or ruptures, the material in the nucleus can squeeze out of the disc or herniate. A disc may herniate a little or a lot, and the symptoms will vary accordingly. A disc herniation usually causes compressive problems if the disc presses against a spinal nerve. The chemicals released by the disc may also inflame the nerve root, causing pain in the area the nerve travels to such as the pelvis, lower back, or legs. If this type of pain travels down the back of the leg, it may be referred to as sciatica.
Disc herniation occurs more often in younger populations (20-50 years old) when the disc is plump and well hydrated. Poor mechanics while lifting heavy objects or making repetitive movements (bending, twisting, and lifting) can place too much pressure on the disc. The increased pressure can cause the annulus to tear and the nucleus to rupture into the spinal canal.
Facet Joint Arthritis
The facet joints along the back of the spinal column link the vertebrae together. They are not meant to bear much weight, but instead allow free, flexible, and coordinated movement of the spine. If a disc loses its height as it degenerates, the vertebra above the disc begins to compress toward the one below. This causes the facet joints to press together and bear more weight. Joint (articular) cartilage covers the surfaces where these joints meet. Just as with other joints in the body that are covered with cartilage, such as the hip and knee, the facet joints can develop osteoarthritis if the articular cartilage wears away over time due to systemic or local inflammation. Extra load and localized inflammation of the facet joints, such as that from a collapsing disc, can speed up degeneration in the facet joints. The swelling and inflammation from an arthritic facet joint can be a source of low back pain.
Segmental Instability
Segmental instability means that the vertebral bones within a spinal segment move more than they should. This movement can develop if the disc or the facet joints have degenerated and the neuromuscular system wasn’t able to adequately compensate. Usually the supporting ligaments around the vertebrae have also stretched over time, and fail to support the joint as it normally would.
One form of segmental instability is a condition called spondylolisthesis, where one vertebral body begins to slip forward over the one below it. When a vertebral body slips too far forward it can cause lower back problems. Firstly, slipping of a vertebra can lead to mechanical pain simply because the structures of the spine move around too much and become inflamed. The abnormal movement can also cause nerve pain symptoms if the spinal nerves are squeezed during movement. This is common in young athletes such as gymnasts who train hard without ideal efficiency or proper mechanics while their skeleton is immature. In addition, some people are born with spondylolisthesis that doesn’t present until adulthood. This condition may also occur due to repetitive microtrauma or serious sudden trauma.
Stenosis
Spinal Stenosis
Stenosis means narrowing of a specific structure. Spinal stenosis refers to a condition in which the tube-like area (spinal canal) surrounding the spinal cord becomes narrow or closes in. This usually occurs due to bony spurs encroaching on the area, but may also develop from other issues such as cysts or tumors. The spinal cord ends at L2 of the lumbar spine. Below this level, the spinal canal contains only the spinal nerves that come from the spinal cord. These nerves travel to the pelvis and legs. When stenosis leads to narrowing of the spinal canal, either the spinal cord or the spinal nerves coming from the cord are squeezed inside of the canal. The pressure on the nerves or spinal cord can disrupt the way the nerves work. Depending on whether it is the spinal cord being compressed or the nerves, and which nerves are being compressed, resulting problems can include pain and numbness in the buttocks, genitalia, and legs. Weakness may also arise in the muscles of the lower body that are supplied by those nerves.

Foraminal Stenosis
Spinal nerves exit the spinal cord between the vertebrae in a boney tunnel called the neural foramen. Stenosis can also occur in this region and cause this tunnel to become smaller or collapse due to disc degeneration. Bone spurs may also form in the area. This subsequently squeezes the spinal nerve as it passes through the tunnel— a condition called foraminal stenosis.

Symptoms
Symptoms from low back problems vary. The pain or symptoms they experience depend on a person's overall health condition, which structures are being affected, and many other factors like stress, sleep, diet, mood and their beliefs about their pain or condition. Some of the more common symptoms of low back problems are:
- Low back pain
- Pain spreading into the buttocks and thighs
- Pain radiating from the buttock to the foot
- Back stiffness and reduced range of motion
- Muscle weakness in the hip, thigh, leg, or foot
- Sensory changes (numbness, prickling, or tingling) in the leg, foot, or toes
In some rare cases, symptoms may involve changes in bowel or bladder function. These symptoms are caused by a large disc herniation or tumor that pushes straight back into the spinal canal and puts pressure on the nerves that go to the bowel and bladder. In addition to loss of control of the bowel and bladder, the pressure on these nerves may cause symptoms of low back pain, pain running down the back of both legs, and numbness or tingling in the saddle/genitalia area. Pressure on these nerves is considered a medical emergency as it can lead to permanent paralysis of the bowel and bladder. This condition is called cauda equina syndrome. Immediate surgery to remove pressure from the nerves is required.
Diagnosis
How will my health care provider find out what's causing my problem?
The diagnosis of low back pain begins with a thorough history of your condition. Your physical therapist will ask you questions to find out when you first started having problems, what makes your symptoms worse or better, and how the symptoms affect your daily activity. Your answers will help guide the physical examination. A physical therapist may also ask you to fill out a questionnaire describing your back problems.
After assessing your medical history, your physical therapist will physically examine the muscles and joints of your low back and ask you to move in different directions to determine how your pain is affected. It is important that your physical therapist understands how your back is aligned, finds out where it hurts, and checks which movements improve or worsen your symptoms.
Your physical therapist may also perform some simple tests to check the function of the nerves in your back. These tests are used to measure the sensation, reflexes, and strength in your legs or feet. The information from your medical history and physical examination will help your physical therapist decide what else needs to be evaluated during the examination.
Most people with low back pain will NOT need x-rays or other tests to diagnose and treat their pain. In some cases, if an x-ray or other diagnostic could be helpful, your physical therapist will refer you to a doctor for further diagnostic imaging.
Once your physical examination is complete, your physical therapist at Clarity Physical Therapy & Wellness Center will discuss treatment options with you that will help speed your recovery, so that you can return to your normal lifestyle as quickly as possible. It should be noted again that in many cases, one distinct, single structure that is causing your back pain may not be identified. Low back pain is rarely that simple. However, even if one specific structure cannot be identified as the cause of the pain, this does not mean physical therapy might not be beneficial. On the contrary, most cases of low back pain can be resolved or effectively managed with consistent physical therapy treatment. The treatment regimen will be structured to your individual needs, such as who you are (e.g., age, gender), how your body moves, what your health beliefs are, and what kind of life you live.
Clarity Physical Therapy & Wellness Center provides physical therapist services in Western Springs.
Physician Review
Diagnostic Tests
In a number of low back pain cases, no special diagnostic testing is required to diagnose and treat your back pain. Your doctor or physical therapist will be able to determine what the most probable cause of your pain is from the history of your injury, how you are moving, and from the physical exam. The exact structure causing the pain in your back may be unknown, but this does not preclude treatment to help your pain. A combination of irritated connective tissues, muscles, joints, ligaments, discs, and nerves in the back is often the culprit, so ‘diagnosing’ or naming one single structure is usually futile. Treatment to help your back problem can still be effective without knowing the exact anatomical cause of your pain.
When acute back pain occurs, diagnostic tests are not routine, as diagnostic tests that are completed unnecessarily may produce misleading findings. In numerous interesting studies, patients have demonstrated major structural changes in different back or spinal structures on x-rays in the absence of physical symptoms.
Diagnostic testing for back pain is reserved for cases where:
- The pain is not acting as your physical therapist or doctor would expect
- Your symptoms aren’t resolving with the usual conservative treatment
- Your pain is intense and relentless
- Your pain is affecting your normal functions
- Your symptoms include nerve pains in your leg and foot
You have a suspected serious problem, such as cauda equina syndrome, which refers to disc disruption that is affecting the nerves supplying your bowel and bladder
Radiological Imaging
If diagnostic tests are deemed necessary, there are several different tests that your doctor may recommend. Radiological imaging tests allow your doctor to see the anatomy of your spine, which assists the determination of what may be causing your back pain. Knowing what structures may be contributing to your back pain may help further direct the most appropriate treatment to assist you.
X-rays
X-rays are usually the first test ordered before any of the more specialized tests are completed. X-rays use electromagnetic radiation to show problems with bones and can also reveal problems such as fractures, infections, or bone tumors. X-rays of the spine can give your doctor information about bone alignment and can demonstrate how much degeneration has occurred in the spine. Both alignment and degeneration can affect the amount of space in the neural foramina and between the discs, which subsequently impacts the nerves in the area. This is important information your health care professional can use to establish a treatment plan.
Flexion and Extension X-rays
Special x-rays called flexion and extension x-rays may help to determine if there is true instability between vertebrae. These x-rays are taken from the side as you bend as far forward and then as far backward as you can. Comparing the two x-rays allows the doctor to see how much motion occurs between each spinal segment.
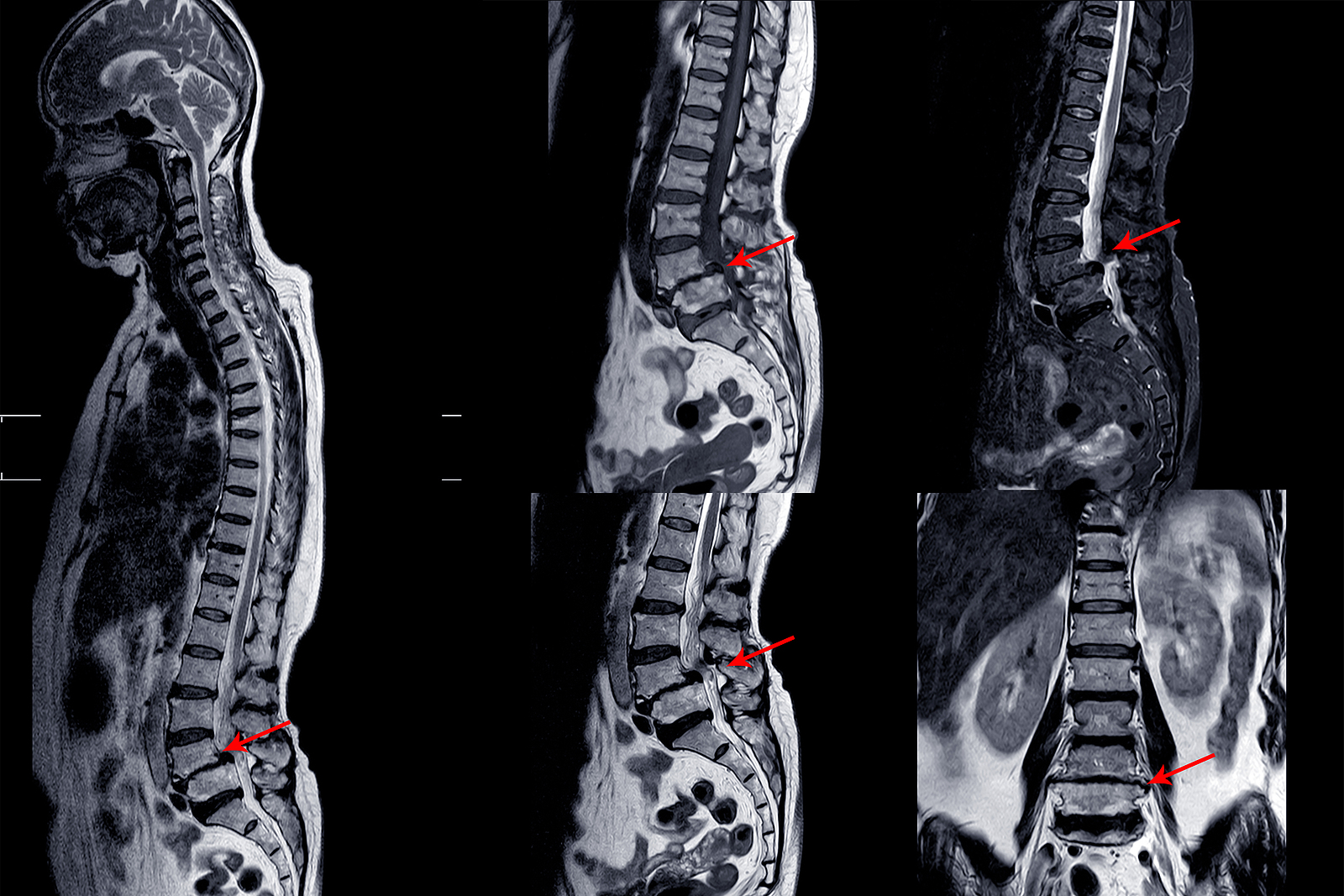
Magnetic Resonance Imaging (MRI)
An MRI scan uses magnetic waves (not radiation) to create pictures of the lumbar spine in sections called slices. The MRI scan shows the bones in the lumbar spine as well as soft tissue structures such as the discs, joints, and nerves. MRI scans are painless and don’t subject you to radiation as an x-ray does. MRI scans are the most common test for visualizing the lumbar spine after an x-ray has been taken. These tests may be recommended if your health care provider is concerned that surgery may be necessary.
In some cases, specialized MRIs that involve an injection of contrast dye may be recommended by your doctor to see specific structures. These special MRIs are performed following the intravenous injection of gadolinium-based dye. The contrast dye enhances image quality and can define some structures more than a regular MRI.
Computed Tomography (CT) Scan
A CT scan is a special type of x-ray that lets doctors see thin sections or slices of tissue. The machine uses a computer and a series of x-rays to create these slices. CT scans subject patients to significantly more electromagnetic radiation than a traditional x-ray, so this type of test will only be ordered when truly necessary to help diagnose a problem. CTs can be useful for the visualization of bones, soft tissues, and blood vessels.
Myelogram
The myelogram is a special kind of x-ray or CT scan where a dye is injected directly into the spinal canal to look for problems in this area. Myelograms are used to help diagnose herniated discs, pressure on the spinal cord or spinal nerves, spinal tumor, or bone spurs that may be pressing on the spinal canal structures.
Discogram
The discogram is another type of specialized x-ray. A discogram has two stages. First, a needle is inserted into the problem disc and then saline is injected to create pressure inside the disc. If this injection reproduces your pain, it suggests that the disc is the source of your problem. During the second part of the test, dye is injected into the disc. The dye can be seen on an x-ray. Using both regular x-rays and CT scan images, the dye outlines the inside of the disc. This can show abnormalities of the nucleus such as annular tears and ruptures of the disc.
Bone Scan
A bone scan (skeletal scintigraphy) specifically diagnoses problems with your bones. During a bone scan, a safe and small amount of a radioactive tracer is injected into your veins. This tracer is taken up by your bones. The tracer illuminates on special diagnostic images taken of your back. The tracer builds up more in areas where bone is undergoing a rapid repair process, such as a healing fracture or the area surrounding an infection or tumor. A bone scan may initially be used to locate a problem, then additional tests such as a CT scan or MRI can be used to look at the area in more detail.
Electromyogram (EMG)
An EMG is a special test used to determine if there are problems with any of the nerves traveling from the spinal cord to the lower limbs. EMGs are usually performed to determine whether the nerve roots have been pinched by a herniated disc or structurally damaged by inflammation. During the test, small needles are placed into certain muscles that are supplied by each nerve root. If there has been a change in the function of the nerve, the muscle will not fire properly and this discrepancy will be noted. Furthermore, an EMG can help determine which nerve root is involved. Often, the nerve disruption has to be significant to show a change on an EMG.
Additional Tests
Not all causes of low back pain are from conditions within the spine itself. Other conditions, such as rheumatoid arthritis, spondyloarthropathies, or an infection may lead to a back problem. Pain may also be referred from issues such as gastrointestinal distress, stomach ulcers, kidney problems, and aneurysms of the aorta. Blood tests, urinalysis, or additional tests may be needed to rule out problems that do not involve the spine.
Physician Treatment
In certain low back pain cases that don’t respond to physical therapy, more aggressive forms of treatment may be required in addition to your active mobility and strengthening program. These are temporary measures and interventions designed to provide short-term relief that allows you to move more and build up your conditioning as well as load tolerance.
Injection-Based Treatments
Spinal injections are used for both diagnostic purposes as well as treatment. There are several different types of spinal injections that your doctor may recommend. Most injections use a mixture of an anesthetic and some type of cortisone (anti-inflammatory) preparation. The anesthetic is a medication that numbs the area where it is injected. If the injection takes away your pain immediately, this provides important information suggesting that the injected area is indeed the source of your pain. The cortisone component in the injection decreases inflammation and can reduce the pain from an inflamed nerve or joint for a prolonged period of time.
Some injections are more difficult to perform and require the use of a fluoroscope. A fluoroscope is a special type of x-ray that allows the doctor to see a real-time x-ray image continuously on a TV screen during the procedure. The fluoroscope is used to guide the needle into the correct place before an injection is administered.
Epidural Steroid Injection (ESI)
Back pain from inflamed nerve roots and facet joints may benefit from an ESI. During this procedure, the medication mixture is injected under fluoroscopy into the epidural space around the nerve roots. Generally, an ESI is only administered when other non-operative treatments aren't working. ESIs are unfortunately not always successful in relieving pain. If they do work, they may only provide temporary relief.
Selective Nerve Root Injection
This type of injection places steroid medication around a specific inflamed nerve root. A fluoroscope is used to guide a needle directly to the affected spinal nerve root, which is then bathed with the medication. In difficult cases, the selective nerve root injection can also help surgeons decide which nerve root is causing the problem before surgery is planned.
Facet Joint Injection
If facet joint inflammation or injury is the suspected cause of the low back pain, an injection into one or more facet joints can help ease pain and more specifically determine which joints are causing the problem.
During this procedure, a fluoroscope is used to guide a needle directly into the facet joint. The facet joint is then filled with a medication mixture. If the injection immediately eases the pain, it helps confirm that the facet joint is a source of pain. The steroid medication will reduce the inflammation in the joint over a period of days and may reduce or eliminate your back pain.
Trigger Point Injections
Injections of anesthetic medications mixed with cortisone are sometimes administered directly into the painful points of muscles, ligaments, or other soft tissues near the spine. These injections can help relieve back pain, muscle spasms, and tender points in the back muscles.
Prolotherapy
Injections of a dextrose-based solution into joints that are moving too freely can be used to stimulate temporary, low-grade local inflammation at the problem area. This initiates a subsequent healing cascade and scarring at the joint, which appears to ‘tighten’ tissue in the affected area. Prolotherapy is not generally performed under fluoroscopy.
Surgery
Surgery for low back pain is, in most cases, a last resort for treatment, except in the case of cauda equina. Surgeons generally prefer that patients try nonsurgical treatments for a minimum of three months before considering surgery. Fortunately, most people with back pain gradually get better with physical therapy. Even people who have degenerative spinal changes tend to gradually improve with time. Only 1-3% of patients with degenerative lumbar conditions typically require surgery. In some stubborn cases of severe back pain that are not improving with physical therapy, surgery may be recommended.
In some rare cases, your doctor may need to perform immediate surgery if you are losing control of your bowels and bladder (cauda equina syndrome) or if your muscles are rapidly becoming weaker. If these conditions develop, surgery is imminently required to remove pressure from specific nerves in your lower back before they become permanently damaged.
There are many different operations that are performed for back pain. The goal of nearly all spine operations is to remove pressure from the nerves of the spine, stop excessive motion between two or more vertebrae, or both. The type of surgery performed depends on each patient's conditions and symptoms.
Laminectomy
The lamina is part of the bony ring of the spinal canal. It forms a roof-like structure over the back of the spinal column. When the nerves in the spinal canal are being squeezed by a herniated disc or from bone spurs pushing into the canal, a laminectomy removes part or all of the lamina to release pressure on the spinal nerves. This is sometimes called a posterior decompression surgery.
Discectomy
When the intervertebral disc has ruptured, the portion that has ruptured into the spinal canal may acutely irritate or compress the nerve roots. This may cause pain, weakness, and numbness that radiates into one or both legs. The operation to remove the portion of the disc that is pressing on the nerve roots is called a discectomy or microdiscectomy. This operation is performed through an incision in the low back immediately over the disc that has ruptured and is one of the most common types of surgeries used to alleviate back pain.
In the past, spinal surgery required a large incision down the affected portion of the spine. Fortunately, spine surgeons can now perform most discectomy procedures through very small incisions in the low back. These surgeries are called minimally invasive surgeries. The obvious advantage of these minimally invasive procedures is there is less damage to the muscles of the back and thus a quicker recovery. Many surgeons are now performing minimally invasive discectomies as an outpatient procedure where no hospital stay is required.
Lumbar Fusion
When there is extra movement between two or more vertebrae, the excess motion can cause pain due to the motion itself as well as irritation of the nerves of the lumbar spine. In these cases, if physical therapy has not helped, a spinal fusion is usually recommended. The goal of a spinal fusion is to force two or more vertebrae to grow together, or fuse, into one bone. A solid fusion between two vertebrae stops the movement between the two bones and pain is reduced because the fusion stops movement and decreases the irritation of the nerve roots. There are many different types of spinal fusions performed.
In the past, the traditional operation to perform a fusion of the lumbar spine involved a procedure in which surgeons ‘decorticated’ the back surface of the vertebrae. Decorticate means to remove the hard outside covering of a bone to create a bleeding bone surface. Once this was performed, a bone graft was taken from the pelvis and laid on top of the decorticated vertebrae. Just like a bone fracture would naturally heal, the bone graft and the bleeding bone grow together and fuse to create one solid bone.
Unfortunately, spinal fusions in the past were not always successful, mainly because the vertebrae failed to fuse together in up to 20 percent of cases. Due to this common failure, surgeons began looking for ways to increase the success of fusions. Since metal plates and screws had been used to treat fractures of other bones for many years, surgeons explored the idea of using metal implants to help fuse spinal segments. The more firmly two bones can be held together while the healing phase occurs, the more likely the bones are to fully heal.
Major advances have been made in recent years in the development of metal rods, metal plates, and special screws that are designed to hold vertebrae together to aid spinal fusion. These new spinal fusion techniques are referred to as instrumented fusions because of the special devices used to secure the vertebrae to be fused. Today the most common type of fusion is performed using special screws called pedicle screws that are inserted into each vertebra and connected to either a metal plate or metal rod along the back of the spine. The vertebrae are still decorticated and the bone graft is still used to stimulate the fusion of bones as they heal. Metal cages are sometimes used to create space in the spine and hold vertebrae in place while natural bone healing and fusion occurs. Depending on the problem, surgeons may need to make a surgical incision in your back or they may need to perform the surgery from your abdominal area.
Our Treatment
What can be done to relieve my symptoms?
Non-surgical Rehabilitation
Whenever possible, it is preferable to use treatments other than surgery. The first goal of these nonsurgical treatments is to ease your pain and other symptoms.
Physical therapy and Exercise
In addition to other nonsurgical treatments, patients with back pain often work with a physical therapist. Physical therapy treatments focus on relieving pain, improving back movement, and fostering healthy posture. Our physical therapist can design a rehabilitation program to address a particular condition and to help you prevent future problems. There is a great deal of scientific evidence that exercise and increased overall fitness reduce the risk of developing back pain and can improve the symptoms of back pain once it begins.
Although the time required for rehabilitation varies among patients, you can expect to continue therapy for two to four months for chronic back problems. Our treatments are designed to ease pain and to improve your mobility, strength, posture, and function. Your physical therapist at Clarity Physical Therapy & Wellness Center will also teach you how to control your symptoms and how to protect your spine for the years ahead.
During your first visit our physical therapist will carefully conduct an evaluation of your current episode of signs and symptoms. This will include a subjective history of the current complaint and a systems review, followed by a thorough objective assessment of your active, passive and physiological movements of your spine and related extremities, including muscular strength and length testing, to identify dysfunction. Our %physiotherpists% have completed extensive training in orthopedic manual therapy and have years of expierence with diagnosing and treating musculoskeletal conditions. By the end of your evaluation your plan of care and what you can expect from your treatments will be clearly outlined.
Our treatment approach is centered around the combination of passive and active therapies. Passive therapies include soft tissue mobilization, myofascial release, joint mobilization/manipulation, modalities, trigger point release and dry needling. These passive treatments are aimed at the restoration of muscle length, the reduction of myofascial guarding and the improvement of physiologic joint mobility. Active therapies include dose exercise progressions, active stretching, postural stabilization, active biofeedback, and strength training. It is very important that our patients understand that both the passive and active treatments are imperative to a successful rehabilitation.
You may be tempted to limit your activity because of your back pain. However, as a result of pain and inactivity, your muscles may become weak and deconditioned, and your back won't function optimally. Physical therapists at Clarity Physical Therapy & Wellness Center in Western Springs use active rehabilitation to prevent the harmful effects of deconditioning. With this active approach, you'll be shown how to lift and move safely. And you'll be shown how to strengthen your back muscles. In addition, aerobic exercises are used to improve your general fitness and endurance.
Aerobic exercises may include walking on a treadmill, riding a stationary bike, or swimming. These activities can relieve the stress of low back pain, and they can cause your body to release endorphins into the blood stream. Endorphins are your body's own natural painkillers.
An active approach to physical therapy can help you attain better muscle function, so you can get your activities done easier. Active rehabilitation speeds recovery, reducing the possibility that back pain will become a chronic problem. Activity helps you resume your normal lifestyle as swiftly as possible. Though you'll be cautioned about trying to do too much, too quickly, you'll be guided toward a return to your usual activities. This approach gives you a greater sense of control. You'll take an active role in learning how to care for your back pain. Clarity Physical Therapy & Wellness Center treatment sessions focus on reassuring you that getting back to work and other normal activities swiftly won't cause you harm and can actually help you get better faster.
When needed, your physical therapist in Western Springs will encourage you to take certain actions to improve your spine health. For example, if you smoke, you'll be encouraged to get help to quit. Because of the limited blood supply in the tissues of the low back, smoking speeds the degenerative process and impairs healing. If you're out of shape, you'll be encouraged to get fit. This strategy makes it less likely that back pain or injury will strike again in the future.
Our physical therapist will show you how to keep your spine safe during routine activities. You'll learn about healthy posture and how posture relates to the future health of your spine. And you'll learn about body mechanics, how the body moves and functions during activity. Your Clarity Physical Therapy & Wellness Center physical therapist will also teach safe body mechanics to help you protect your low back as you go about your day. This includes the use of safe positions and movements while lifting and carrying, standing and walking, and performing work duties.
As you recover, our physical therapist will gradually advance your treatment in a series of strengthening exercises for the abdominal and low back muscles. Working these core muscles can help you begin moving easier and lessens the chances of future pain and problems.
As our rehabilitation program evolves, you will progress with more challenging exercises. The goal is to safely advance your strength and function.
Your physical therapist will work closely with your doctor and employer to help you get back on the job as quickly as reasonably possible. You may be required to do lighter duties at first, but as soon as you are able, you'll begin doing your normal work activities. We can also do a work assessment to make sure you'll be safe to do your job. Our physical therapist may suggest changes that could help you work safely, with less chance of re-injuring your back.
Back Brace
A back support belt is sometimes recommended when back pain first strikes. It can help provide support and lower the pressure inside a problem disc. Clarity Physical Therapy & Wellness Center patients recovering from back pain are encouraged to gradually discontinue wearing the support belt over a period of two to four days. Otherwise, back muscles begin to rely on the belt and start to shrink (atrophy).
Medications
Ensure that you consult with your doctor or pharmacist regarding the use of pain relief or anti-inflammatory medication. Many different types of medications are typically prescribed to help gain control of the symptoms of low back pain. There is no medication that will cure low back pain. Medications are prescribed to help with sleep disturbances and to help control pain, inflammation, and muscle spasm.
Post-surgical Rehabilitation
Rehabilitation after surgery is much more complex. Depending on what operation you've had, you may leave the hospital shortly after surgery. Some procedures, such as fusion surgery, require that you stay in the hospital for a few days.
During recovery from surgery, you should follow your surgeon's instructions about wearing a back brace or soft lumbar support belt. You should be cautious about overdoing activities in the first few weeks after surgery.
You may need physical therapy outside of the hospital. If you had a lumbar fusion, your surgeon may have you wait six weeks to three months before starting physical therapy. Although the time required for recovery varies, once you start physical therapy, you'll usually go for one to three months, depending on your progress and the type of surgery you had.
When you first visit Clarity Physical Therapy & Wellness Center after surgery, our physical therapist may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm pain and muscle spasm. Pool therapy is often helpful after lumbar surgery.
We will use exercises are used to improve flexibility in your trunk and lower limbs. Strengthening for your abdominal and low back muscles is started. Our physical therapist will instruct you in safe ways to sleep, sit, lift, and carry. And you’ll be given ideas on how to do your work activities safely.
Ideally, you'll be able to go back to your previous activities. However, you may need to modify your activities to avoid future problems.
When treatment is well under way, regular visits to Clarity Physical Therapy & Wellness Center will end. Although we will continue to be a resource, you'll be in charge of doing your exercises as part of an ongoing home program.
Clarity Physical Therapy & Wellness Center provides services for physical therapy in Western Springs.